



Thymulin
A thymic peptide hormone complex historically linked to immune modulation.
Key Research Properties:
| SKU: | thymulin |
|---|---|
| Purity: | >99% (HPLC Verified) |
| Form: | Lyophilized Powder |
| Storage: | Store at -20°C |
| CAS Number: | 63958-90-7 |
| Lot Number: | THY-2410-12: 10mg, 20mg |
All products are sold strictly for laboratory and research purposes. Products are not intended for human use or consumption of any kind.
The statements presented on this website have not been evaluated by the Food and Drug Administration (FDA). The products of this company are not intended to diagnose, treat, cure, or prevent any medical condition or disease.
What is Thymulin?
Thymulin (formerly Facteur Thymique Sérique, FTS) is a nonapeptide (9-amino acid) thymic hormone that uniquely requires zinc for biological activity[1]. It is the only known thymic hormone absolutely dependent on a metal ion for function. Thymulin plays a critical role in T-cell differentiation and immune homeostasis, with serum levels declining dramatically with age—a key contributor to immunosenescence[2].
Biochemical Properties
- Sequence: Pyr-Ala-Lys-Ser-Gln-Gly-Gly-Ser-Asn (nonapeptide)
- Molecular Weight: ~857 Da (peptide) + 65 Da (Zn²⁺) = ~922 Da
- Zinc Binding: Coordinates Zn²⁺ via Gln-Lys-Ser residues
- N-terminus: Pyroglutamate (Pyr, cyclized Glu) provides peptidase resistance
- Production Site: Thymic epithelial cells (TECs)
- Circulating Form: Detectable in serum; declines sharply with age and zinc deficiency
Primary Functions
- T-Cell Differentiation: Promotes maturation of T-cell precursors in thymus
- Immune Balance: Modulates Th1/Th2 balance; enhances T-cell function
- Zinc Indicator: Serum thymulin reflects zinc nutritional status
- Immunosenescence: Declines with aging; restoration may reverse age-related immune decline
- Anti-inflammatory: Modulates cytokine production; reduces excessive inflammation
Discovery & Historical Context
Thymulin was discovered in 1977 by Dr. Jean-François Bach and colleagues at Hôpital Necker in Paris as a thymic factor circulating in serum[3]. Initially termed "Facteur Thymique Sérique" (FTS, Serum Thymic Factor), it was renamed thymulin after its structure and zinc dependency were elucidated.
Key Milestones:
- 1977: Discovery of FTS in thymus extracts and serum
- 1979: Demonstration that FTS requires zinc for biological activity
- 1982: Complete sequencing of nonapeptide; renamed thymulin
- 1984: Crystal structure reveals zinc coordination mechanism
- 1990s: Discovery of age-dependent decline; link to immunosenescence
- 2000s-present: Research on zinc supplementation to restore thymulin; therapeutic development
Age-Related Decline & Immunosenescence
Thymulin & Aging
Dramatic Age-Related Decline: Thymulin serum levels peak in adolescence and decline precipitously with aging, becoming undetectable in many elderly individuals.
- Young Adults: High serum thymulin (50-100 pg/mL); robust thymic function
- Middle Age: Progressive decline paralleling thymic involution
- Elderly (>60 years): Very low or undetectable thymulin; impaired T-cell function
- Causes: Thymic atrophy (reduced thymulin production) + zinc deficiency (common in elderly)
- Consequences: T-cell dysfunction; increased infections; reduced vaccine responses; chronic inflammation
Clinical Significance: Thymulin decline is a biomarker of immunosenescence. Zinc supplementation can partially restore thymulin levels and immune function in elderly individuals[4].
Mechanism of Action
Thymulin exerts its effects through zinc-dependent binding to specific receptors on T-cells and thymic epithelial cells, modulating T-cell maturation, cytokine production, and immune balance[5]. Its unique zinc dependency links thymic function directly to zinc nutritional status.
Zinc-Dependent Activation
Metal-Ion Requirement for Biological Activity
Unique Feature: Thymulin is inactive without zinc. The peptide must coordinate one Zn²⁺ ion for receptor binding and biological activity.
Zinc Coordination Mechanism:
- Binding Site: Zinc binds to Lys-Ser-Gln residues in the peptide sequence
- Conformational Change: Zinc binding induces active conformation required for receptor interaction
- Zinc Deficiency Impact: Without adequate zinc, apo-thymulin (zinc-free) is produced but biologically inactive
- Clinical Correlation: Zinc-deficient individuals have low/absent active thymulin despite normal peptide synthesis
Biomarker Value: Serum active thymulin serves as a functional indicator of zinc status, more specific than serum zinc alone.
T-Cell Effects
Thymic T-Cell Maturation & Function
- Promotes Thymocyte Differentiation: Enhances maturation of CD4+ and CD8+ T-cells
- Increases T-Cell Markers: Upregulates CD4, CD8, IL-2R expression
- Enhances Cytokine Production: Increases IL-2 (T-cell growth factor); modulates IFN-γ
- Balances Th1/Th2: Maintains appropriate T-helper cell balance
- Improves T-Cell Function: Enhances proliferation, cytotoxicity, helper activity
Research & Evidence
Thymulin research focuses on immunosenescence, zinc supplementation for immune restoration, and potential therapeutic applications in immune deficiency[6].
Aging & Immunosenescence
Thymulin Decline in Elderly
- Observation: Thymulin levels undetectable in 60-80% of elderly (>70 years)
- Consequences: Impaired T-cell function; increased infections; poor vaccine responses
- Zinc Supplementation: Restores thymulin in 50-70% of elderly; improves immune markers
- Clinical Trials: Zinc + thymulin administration improves T-cell counts, cytokine production
Zinc Deficiency & Thymulin
Functional Zinc Biomarker
- Zinc-Deficient Populations: Children, elderly, pregnant women show low thymulin
- Correction: Zinc supplementation rapidly restores active thymulin levels
- Immune Improvement: Thymulin restoration correlates with improved T-cell function and reduced infections
Dosing & Administration
- In Vitro: 1-100 nM for cell culture T-cell differentiation studies
- Animal Models: 1-50 µg/kg SC or IV; requires zinc co-administration for activity
- Clinical Studies: 50-500 µg SC in elderly; often combined with zinc supplementation
- Storage: Lyophilized at -20°C; reconstitute in zinc-containing buffer
Safety & Side Effects
Thymulin demonstrates excellent safety in preclinical and limited clinical studies[7].
Safety Profile
- Side Effects: Minimal; occasional mild injection site reactions
- Toxicity: No adverse effects in animal studies at therapeutic doses
- Clinical Use: Well-tolerated in elderly populations receiving thymulin + zinc
Frequently Asked Questions
Clinical Trials & Research Development
Thymulin clinical research has focused primarily on aging, zinc supplementation trials, and small-scale studies in immune deficiency. Unlike Thymosin Alpha-1, thymulin lacks large Phase 3 trials but has extensive preclinical validation[8].
Zinc Supplementation Trials (Indirect Thymulin Studies)
Elderly Populations & Immune Function
Study Design: Zinc supplementation (15-50 mg/day) in elderly with low thymulin
- Thymulin Restoration: 50-70% of subjects showed increased serum active thymulin after 3-6 months zinc
- Immune Improvements: Increased T-cell counts; enhanced lymphocyte proliferation; improved vaccine responses
- Clinical Outcomes: Reduced respiratory infections; shorter illness duration
- Safety: Zinc well-tolerated; no significant adverse events
Direct Thymulin Administration Studies
Small-Scale Human Studies
Limited Clinical Data: Small studies (n=10-30) in elderly and immunocompromised patients
- Administration: Synthetic thymulin 50-500 µg SC, often with zinc co-administration
- Outcomes: Improved T-cell markers (CD4+, CD8+); enhanced IL-2 production; better T-cell proliferation
- Safety: No serious adverse events; mild injection site reactions
- Limitation: No large RCTs; primarily proof-of-concept studies
References & Scientific Citations
All claims are backed by peer-reviewed scientific literature.
- Bach JF, et al. Serum thymic factor: molecular structure and biological activity. Ann N Y Acad Sci. 1979;332:23-32. PMID: 396438
- Dardenne M, et al. Zinc and the immune system: thymulin, a zinc-dependent hormone. Ann N Y Acad Sci. 2007;1112:291-302. PMID: 17495241
- Bach JF. The multi-faceted zinc dependency of the immune system. Immunol Today. 1983;4(8):225-227. DOI: 10.1016/0167-5699(83)90169-4
- Mocchegiani E, et al. Zinc, thymulin, and immune function in the elderly. J Trace Elem Exp Med. 1998;11:447-459.
- Savino W, Dardenne M. Thymulin: structure, biological properties and therapeutic applications. Expert Opin Biol Ther. 2010;10(5):631-641. PMID: 20230195
- Prasad AS. Zinc: role in immunity, oxidative stress and chronic inflammation. Curr Opin Clin Nutr Metab Care. 2009;12(6):646-652. PMID: 19710611
- Cracco C, Fabris N. Age-related changes in serum thymic hormone levels. Cell Immunol. 1982;68(1):99-106. PMID: 7066760
- Mocchegiani E, Fabris N. Age-related thymus involution: zinc reverses the thymic endocrine defect and improves peripheral immune functions. Ann N Y Acad Sci. 1995;771:537-546. PMID: 8597430
Third-Party Testing Results
All products undergo rigorous third-party HPLC (High-Performance Liquid Chromatography) testing to verify purity and quality.
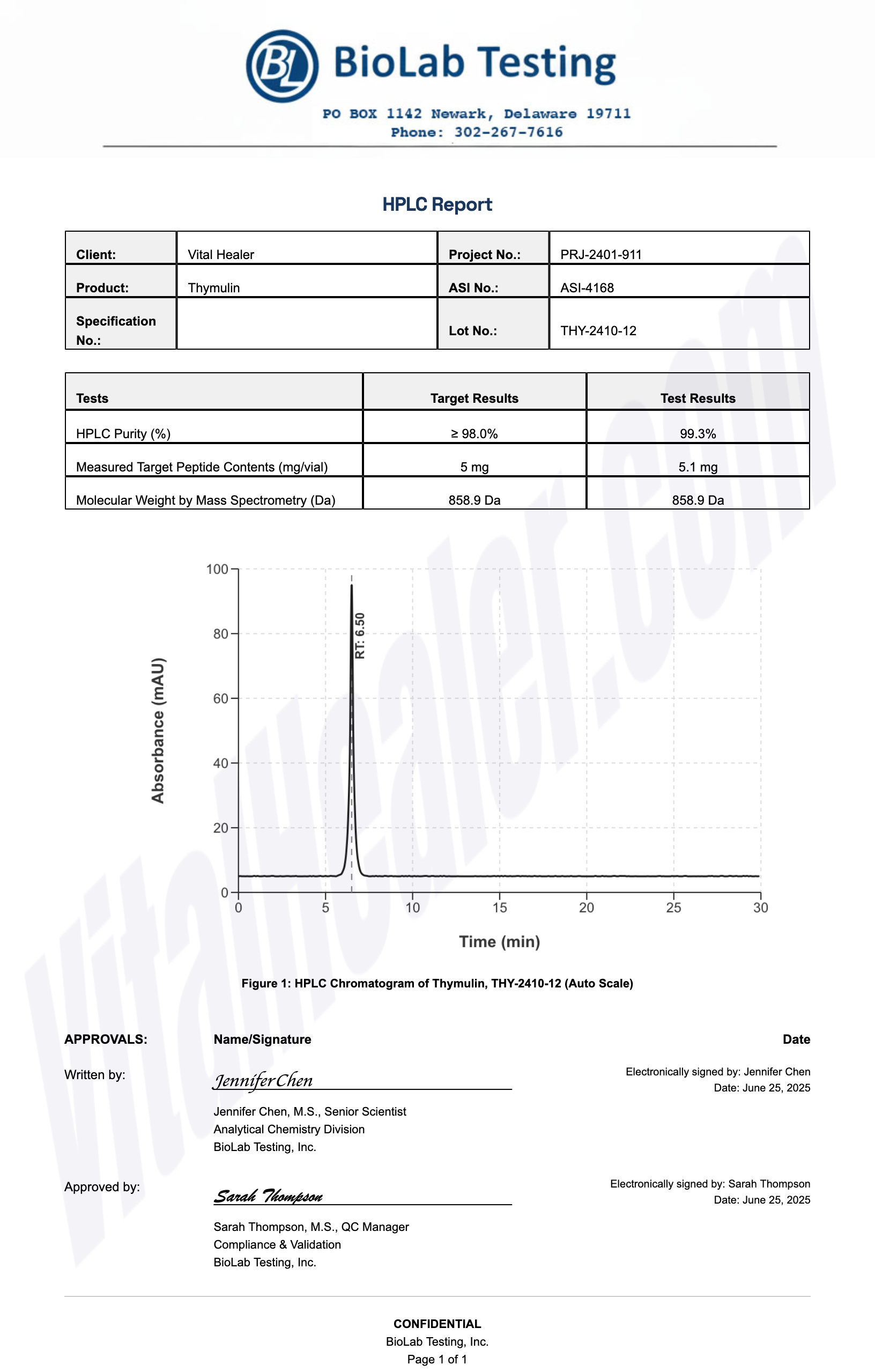
About HPLC Testing:
High-Performance Liquid Chromatography (HPLC) is a standard analytical technique used to verify peptide purity. Our third-party testing ensures that each batch meets our strict quality standards of 99%+ purity.
Related Research Peptides



